

NEUROLOGY
Painful Diabetic Polyneuropathy
Clinical Guidelines and Resources
Sign up for Figure 1 and be notified directly of new clinical cases and related research, CME activities, quizzes, news, and trends. It’s free!
Figure 1, 2, 3
1. Patients with diabetes should be assessed for painful diabetic polyneuropathy and comorbid disorders

2. Painful diabetic polyneuropathy can be treated effectively with medications including TCAs, SNRIs, gabapentinoids, and/or sodium channel blockers

3. Opioids are not recommended for the treatment of painful diabetic polyneuropathy
Summary
Clinicians should assess patients with diabetes for peripheral neuropathic pain, and ask about its effect on their function and quality of life. Patients should be counseled that the goal of medications is to reduce, and not necessarily eliminate, pain. Complete resolution of symptoms at this time is rarely achieved, with 30% pain reduction being considered a success in clinical trials. Discussions are warranted to align patient expectations.
It is helpful to assess for other factors that may affect pain perception and quality of life, including mood and sleep disorders. Treatment of these other factors may reduce pain and improve quality of life.
Painful Diabetic Polyneuropathy Clinical Guidelines and Resources
Diabetic Polyneuropathy Patient Cases
Four classes of oral medications have demonstrated evidence of pain reduction in meta-analyses:
- TCAs
- SNRIs
- Gabapentinoids
- Sodium channel blockers
These should be offered to help reduce pain in painful diabetic neuropathy.
Clinicians may assess patient preferences for effective oral, topical, nontraditional, and nonpharmacologic interventions for painful diabetic neuropathy. For these patients, clinicians may offer topical (capsaicin, glyceryl trinitrate spray, Citrullus colocynthis), nontraditional (Ginkgo biloba), or nonpharmacologic interventions (CBT, exercise, Tai Chi, mindfulness).
As pharmacological agents for painful diabetic neuropathy have similar efficacy, clinicians should consider potential adverse effects, patient comorbidities, cost, and patient preferences, when recommending treatment. In patients of childbearing potential with painful diabetic neuropathy, clinicians should not offer valproic acid.
Clinicians should also counsel patients that a series of medications may need to be tried to identify the treatment that most benefits patients with painful diabetic neuropathy. A typical treatment trial is approximately 12 weeks.
Opioids should not be routinely used for painful diabetic neuropathy, given lack of long-term efficacy and long-term adverse consequences. If patients are on these medications for painful diabetic neuropathy, the options of a safe taper may be presented, as well as discussions of alternative treatment strategies.
Clinicians should not use tramadol and tapentadol (opioids/SNRI dual mechanism agents) for the treatment of painful diabetic neuropathy. If patients are on these medications for painful diabetic neuropathy, the options of a safe taper may be presented, as well as discussions of alternative treatment strategies.
Full Guidelines
Read the most recent full guidelines for clinical management of diabetic polyneuropathy: American Academy of Neurology clinical guidelines on the management of diabetic polyneuropathy.
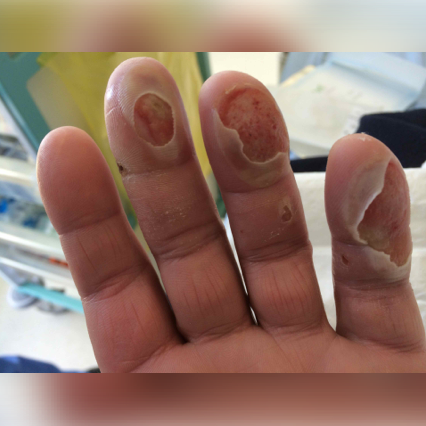
Diabetic Polyneuropathy Patient Cases
Click on the image to see the full case details and sign in to view community comments.



See more cases like these
Sign up for Figure 1 and gain access to a library of 100,000+ real-world cases.

Related Research
Screening, Diagnosis and Management of Diabetic Sensorimotor Polyneuropathy in Clinical Practice: International Expert Consensus Recommendations | PubMed
“Diabetic sensorimotor polyneuropathy (DSPN) affects around one third of people with diabetes and accounts for considerable morbidity, increased risk of mortality, reduced quality of life, and increased health care costs resulting particularly from neuropathic pain and foot ulcers…Considering the individual risk profile, pain management should not only aim at pain relief, but also allow for improvement in quality of sleep, functionality, and general quality of life.”
Peripheral Diabetic Neuropathy | PubMed
“Peripheral neuropathy (PN) encompasses a broad range of clinical pathologies potentially presenting with peripheral nervous system dysfunction. Patients with PN often present with varying degrees of numbness, tingling, and/or burning in the extremities…The exact cause of diabetic peripheral neuropathy is not known. Proposed theories include metabolic, neurovascular, and autoimmune pathways have been proposed. Mechanical compression (e.g., carpal tunnel), genetics, social and lifestyle factors such as chronic alcohol consumption, and smoking all have been implicated.”
Diabetic Polyneuropathy and Carpal Tunnel Syndrome Together Affect Hand Strength, Tactile Sensation and Dexterity in Diabetes Patients | PubMed
“Carpal tunnel syndrome (CTS) and diabetic polyneuropathy (DPN) can occur together, and this concomitance is thought to be higher in diabetes patients. We aimed to examine and compare hand function in type 2 diabetes mellitus patients without CTS and DPN (CTS-DPN-), patients with CTS without DPN (CTS+DPN-), patients with DPN without CTS (CTS-DPN+), and patients with CTS and DPN (CTS+DPN+).”

Related Medical Calculators
PEDIS Score for Diabetic Foot Ulcers

Join Your Colleagues
Sign up for Figure 1 and join the largest global community of healthcare professionals exchanging knowledge in real time.