Learning Objective
- Recognize the risk of subarachnoid hemorrhage in patients with polycystic kidney disease
A 32-year-old patient presents to a hospital in an under-resourced setting with no access to CT or MRI. The patient reports having had a headache at home and then losing consciousness, so was urgently transported to the hospital by family members.
On arrival the patient has a Glasgow Coma Scale score of 4, with an extension posturing response to physical stimuli. The patient is stabilized, intubated, and admitted to the intensive care unit. On physical exam cystic masses are palpated in the abdomen.
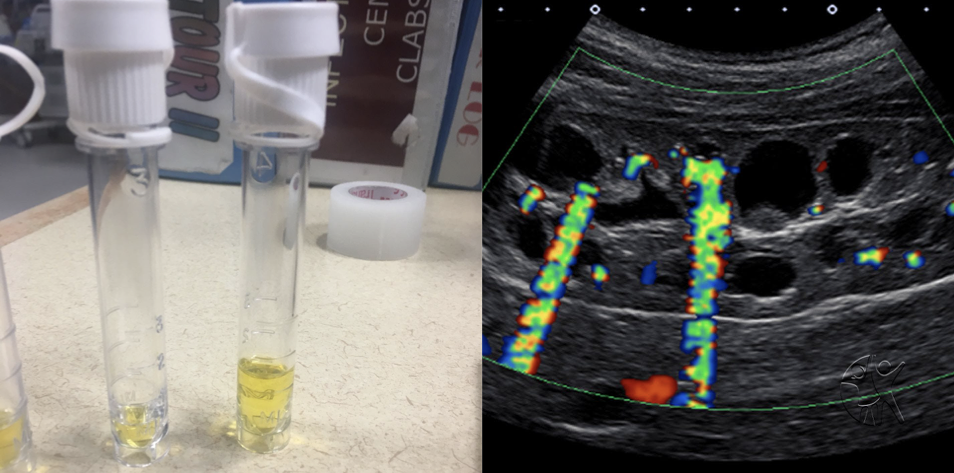
A lumbar puncture reveals many red blood cells and visually assessed xanthochromia after centrifuge. Abdominal ultrasound is performed and reveals the presence of extensive cysts of various sizes within the renal and hepatic parenchyma. The patient is diagnosed with polycystic kidney disease and subarachnoid hemorrhage. The next day, the patient rapidly deteriorates and dies.
Polycystic Kidney Disease and Subarachnoid Hemorrhage Overview
Polycystic kidney disease is often not limited to cysts forming in the kidney, but can include cyst formation in the pancreas, liver, inguinal hernia, cardiac valve disease, diverticula in the colon as well as subarachnoid cysts.
The incidence of subarachnoid cysts with hemorrhage in autosomal dominant adult polycystic disease is between 8-12%, four times higher than the general population. Subarachnoid hemorrhage can be distinguished from a traumatic lumbar puncture by the presence of xanthochromia, with the limitation that the presence of more than 5,000 red blood cells per microliter may also cause xanthochromia over minutes to hours because of continued red blood cell breakdown.
Visual evaluation of xanthochromia is much less reliable than laboratory evaluation if it is available.
Further Reading
References
Abraham MK, Chang WW. Subarachnoid Hemorrhage. Emerg Med Clin North Am. 2016 Nov;34(4):901-916. doi: 10.1016/j.emc.2016.06.011. PMID: 27741994.
Graves P, Sidman R. Xanthochromia is not pathognomonic for subarachnoid hemorrhage. Acad Emerg Med. 2004 Feb;11(2):131-5. PMID: 14759953.
Harris PC, Torres VE. Polycystic kidney disease. Annu Rev Med. 2009;60:321-37. doi: 10.1146/annurev.med.60.101707.125712. PMID: 18947299; PMCID: PMC2834200.
Sanchis IM, Shukoor S, Irazabal MV, Madsen CD, Chebib FT, Hogan MC, El-Zoghby Z, Harris PC, Huston J, Brown RD, Torres VE. Presymptomatic Screening for Intracranial Aneurysms in Patients with Autosomal Dominant Polycystic Kidney Disease. Clin J Am Soc Nephrol. 2019 Aug 7;14(8):1151-1160. doi: 10.2215/CJN.14691218. Epub 2019 Jul 30. PMID: 31362991; PMCID: PMC6682820.
Published December 20, 2023
Want more clinical cases?
Join Figure 1 for free and start securely collaborating with other verified healthcare professionals on more than 100,000 real-world medical cases just like this one.